
- September. A Developmental Pediatrician’s busiest (and most frustrating) time of year.
Back to school anxiety affects just about every child. The buildup to a new environment, people, and studies in the face of decreased ability to communicate, creates a perfect storm for inappropriate or disruptive behaviors in neuro-divergent students.
When an educator proclaims that, “Your child has ADHD and needs medication,” the appropriate response should be, “Stay in your lane!” It would be much more useful if the teacher would explain the signs or symptoms that are troubling and interfere with learning.
What “Professional Psychological Evaluation” doesn’t wind up with Attention Deficit – Hyperactivity Disorder? It’s the same conclusion with same recommendations.
Please… medical diagnoses and treatments should be left to the child’s doctor.
So, what are the actual signs of Attention Deficit – Hyperactivity ‘disorder’ that are concerning?
♦ Overactivity
♦ Learning difficulties
♦ Focus
♦ Attention
♦ Anxiety
♦ Tantrums
♦ Oppositional
What are the possible causes- the differential diagnoses – for this set of symptoms?
Most people over the age 18 years who visit the doctor are usually subjected to a full set of “labs”; testing to help discover the reasons for coming to the practitioner and assuring that any medication(s) will be safe and physically tolerated.
The answer that pediatricians, neurologists, psychologists and psychiatrists commonly offer about your child with challenging behaviors is, “Oh, It’s ADHD – medication will get that addressed.”
Is that good medicine?
Laboratory Testing
The most troubling results that we uncover are Vitamin D3 deficiency, iron deficiency, anemia, certain food intolerances, thyroid issues, cholesterol abnormalities, and gastro-intestinal dysbiosis (including bad bacteria, parasites and fungus-yeast).
Even if the patient does eventually require medication to address signs and symptoms, who can argue that the dosing and effectiveness would not be enhanced by good health?
Behaviors
The primary behavioral issues that we encounter include weak processing-> poor focus -> anxiety -> fidgeting -> more anxiety -> inattention -> easily distracted -> ADHD diagnosis.
Digital devices, which amplify repetitive behaviors and social isolation are frequently inappropriately utilized to get a patient to stay still.
Importantly, the amount of time that the patient spends NOT interacting with peers will certainly impact the maturity level.
Treatments
1. Diet and exercise. Yeah, I know. Your kid is a picky eater and doesn’t like to go outside.
2. Special diets, starting with lower refined sugars and more natural foods. This can be a potent intervention. At least, the healthier child will respond to lower doses of medication and may not require frequent alterations.
3. Omega-3 oils in various combinations are often a helpful, non-addictive supplement for focus and attention.
4. Low Dose Naltrexone has been discussed elsewhere in this forum. This intervention, and the more potent pharmacologic choice, such as Guanfacine (Intuniv), would help because of anxiety reduction that leads to improved attention and focus.
5. Stimulant medications, starting with methylphenidates (e.g. Concerta or Focalin) and moving on to methamphetamines, such as Adderall.
6. Psychiatric medications, such as Prozac, Zoloft, and Risperidone, with even more risk and sometimes poor reactions and side effects.
It is at this point that families may come to realize that their extremely intelligent child needs something other than a parade of medications with variable results and only mild or short-lived improvements.
Please, someone tell me what ADHD has to do with why your 5-year-old is standing on his head or licking the bottom of a table? Why is the child spinning strings with both hands and focusing on that activity? How frequently do the patients have difficulties with gross and fine motor tasks? Walking on toes? And why are sensory issues so prominent or speech was slow to develop?
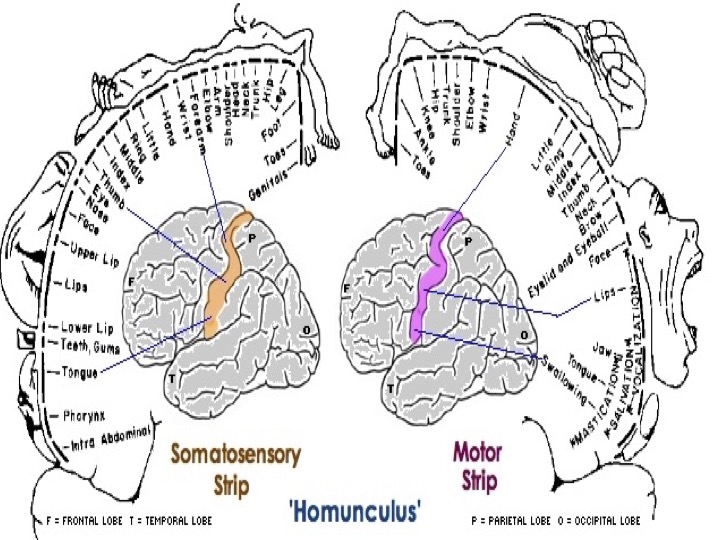
Imagine the motor strip to be activated over and over without properly exciting the portions of the brain that control vocalization, lips and tongue. That patient would be flapping hands, opening the mouth, biting and teeth grinding. Some impulses may not even go that far, so the individual gets on their toes. And, if an impulse doesn’t even reach the motor strip and excites the sensory strip, over-reaction to sound, sight and touch becomes the visible problem.
The experience at The Child Development Center has shown that utilizing “B” vitamin protocols, including methyl B12 via injection or oral, glutathione and various forms of folinic acid, leads to better processing. The result of that improved signaling is evidenced by ‘surprising’ improvements that may appear and re-appear, and then sustained improvements in language and communication, leading to interaction with peers.
This form of intervention into the ADHD diagnosis takes a lot more time, some expense and patience than stuffing a child with potent pharmaceuticals. The side effect of leucovorin (folinic acid) increasing impulses in the brain is – INCREASED activity. The biggest obstacle to advancing the protocol is underlying inflammation, in which activating vitamins would be fueling the fire. That means that the patient must be in the optimal state of health, given supplements to address anxiety and a healthy gut, starting with low doses of important vitamins and increasing very slowly.
The next step… conversation with peers, requires impulses traveling from the speech areas to the frontal lobe, where thought and intelligence are demonstrated. Until better protocols come along, that will take more patience, vigilance, and B-vitamins with Folinic acid. Then, watch the “ADHD” diagnosis becomes more clear as a function of the apraxia (difficulty controlling many muscles) and conversations about more potent medications take a back seat.![]()
![]()
I’ve read several just right stuff here. Certainly price bookmarking for revisiting. I wonder how a lot effort you place to create this kind of great informative website.